Plantar fasciopathy
Description
Plantar fasciopathy is a well-known condition where the plantar fascia is placed under an excessive load and results in micro-tearing and overuse changes of the tissue. Plantar fascial pathologies are documented as a multi-factorial condition, however biomechanically are considered to be resultant of a compression or tension pathology.
Compression
Compression of the medial calcaneal tubercle with significant rearfoot pronation – also noted with other plantar heel conditions, including baxter’s neuritis.
Tension
Considered the cause in plantar fascial pathologies of patients with cavus foot types, restricted posterior chain range of motion or forefoot equinus.
Compression and tension causes may both be present in patients so it is key to identify this through your biomechanical assessment.
Keys to effective plantar fasciopathy orthotic management:
Understanding the compression and tension pathologies is the first step to effective management. Ensuring appropriate offloading of tissue can be achieved through an adequately MLA contouring device with the additional elements addressing the tension / compression elements.
Tension
Knowing tension can be a resultant of increased strain on the posterior chain / plantar fascia – the primary goal is to reduce the overall tensile load during weight bearing. Adding a tapered heel raise (full length, ¾ length or heel only) is an effective way to offload the tension through the plantar fascia.
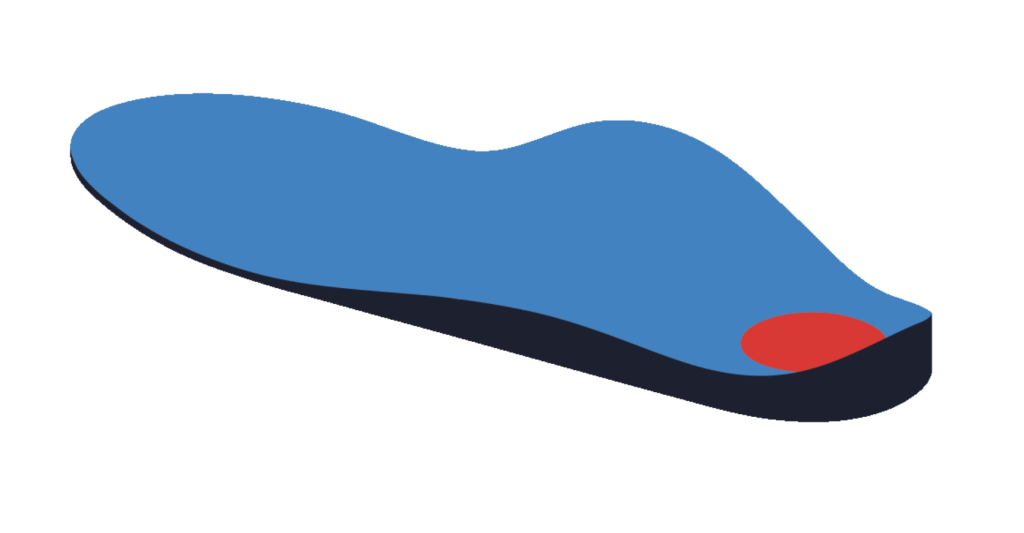
The Extrinsic Heel Lift will be tapered from the proximal heel to no thickness in-line with the sulcus. The specified thickness will be measured from the heel centre as indicated by the pink line in the image below.

It is important to identify whether a patient has a forefoot equinus/anterior cavus as placing a tapered heel raise will increase the forefoot load, and can reduce the effectiveness of offloading. In patients with forefoot equinus utilising a Cuban heel addition extrinsically (designed and applied by OBD) can significantly improve your patients outcomes.
Compression
One element of reducing compression can be achieved through a rearfoot post and adequate MLA contour. Further to this, reducing compression with cushioning can be an effective way to reduce peak pressures around the plantar calcaneal area and medial calcaneal tubercle. This can be achieved with an aperture of the heel filled with a soft poron material.
Apertures can be applied to the orthotic and then filled with a soft material (poron) to provide the patient with relieving padding within the orthotic. The centre of the heel of a Machined EVA orthosis is removed. This region may be filled with a poron material.