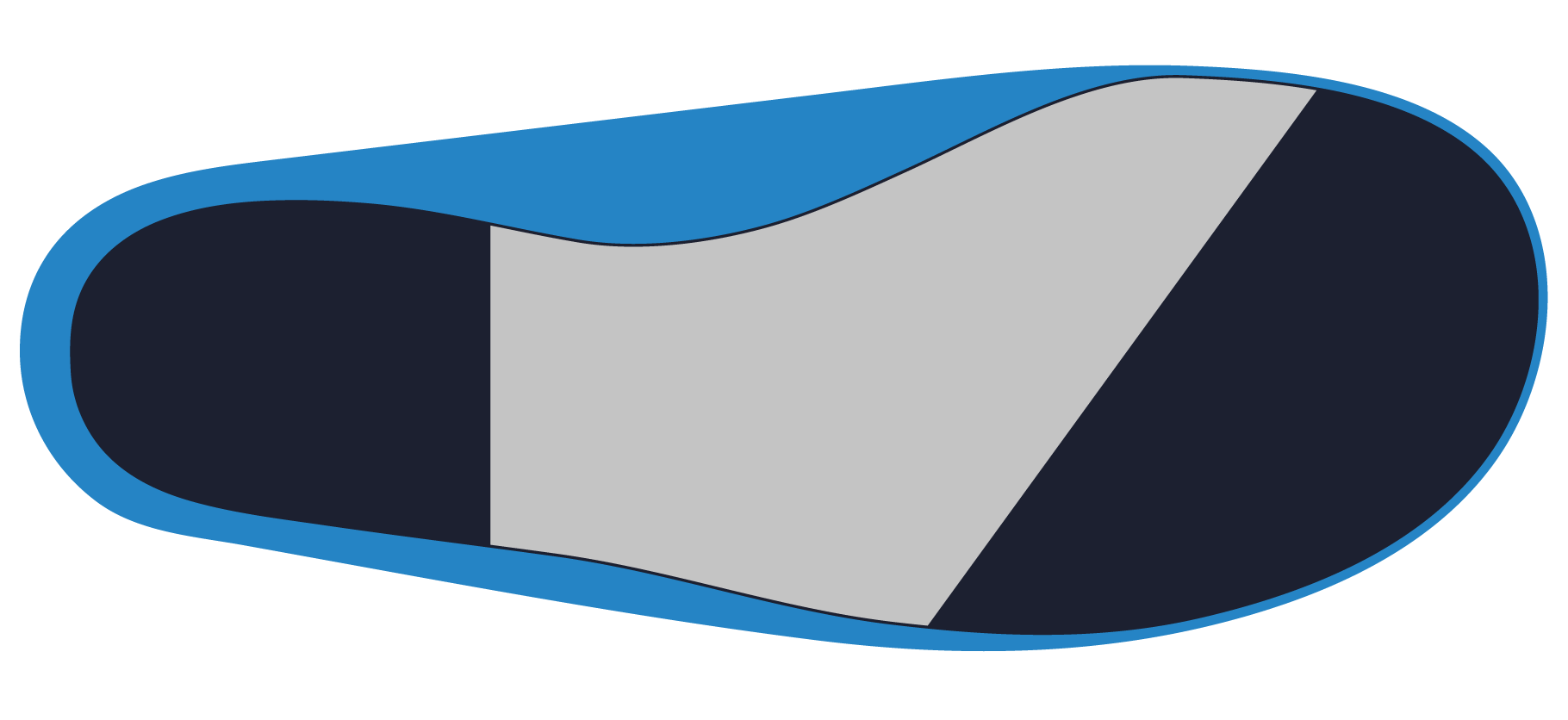
The Extrinsic Heel Lift option allows a user to request a custom EVA wedge be adhered to the plantar surface of the orthosis. The thickness may be customised, as well as the degree of taper and the density of EVA.
| Available Selections | Available Materials | Minimum Value | Maximum Value |
|---|---|---|---|
| Standard Taper | EVA 350 (Default) EVA 400 EVA 260 EVA 220 EVA 190 EVA 125 | 0mm | 30mm |
| Tapered to MPJ’s | 0mm | 30mm | |
| Tapered to Sulcus | 0mm | 30mm | |
| Tapered to Distal Edge | 0mm | 30mm |
Please note that you should contact your laboratory for specific information on the available materials.
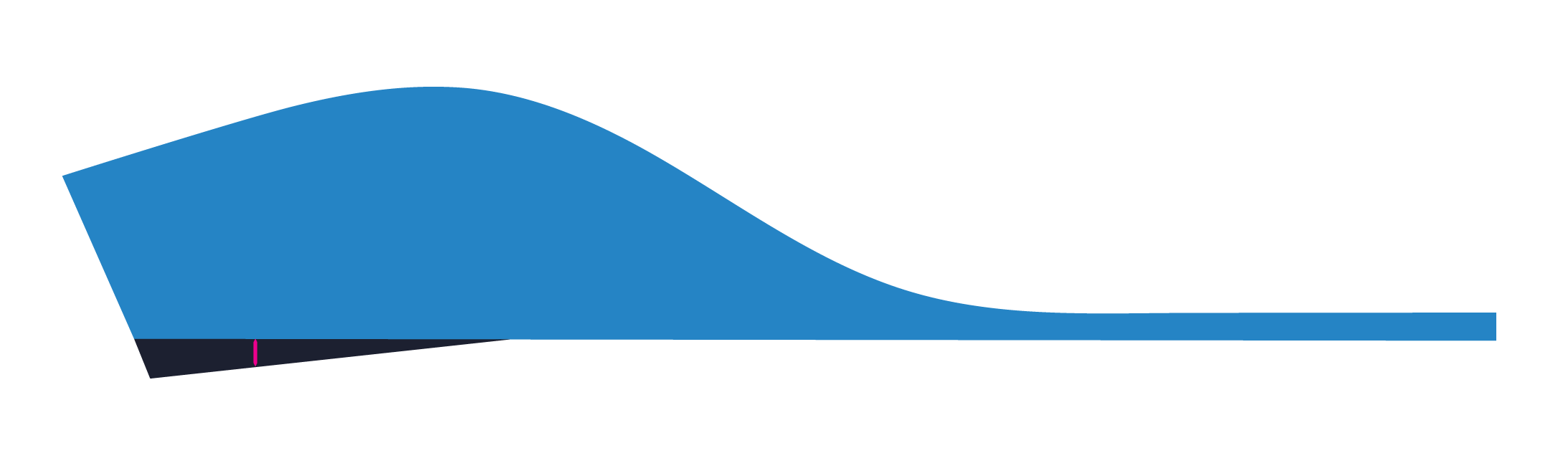
Standard Taper
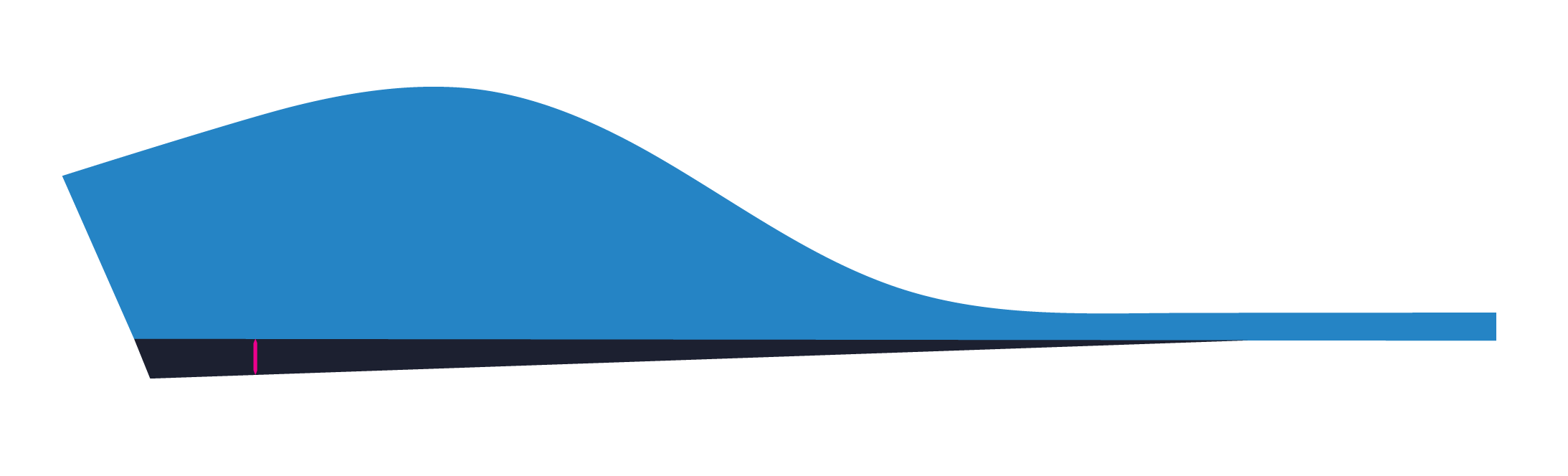
The Extrinsic Heel Lift will be tapered from the proximal heel to no thickness in-line with the peak of the medial longitudinal arch. The specified thickness will be measured from the heel centre as indicated by the pink line in the image below.
Tapered to MPJ’s
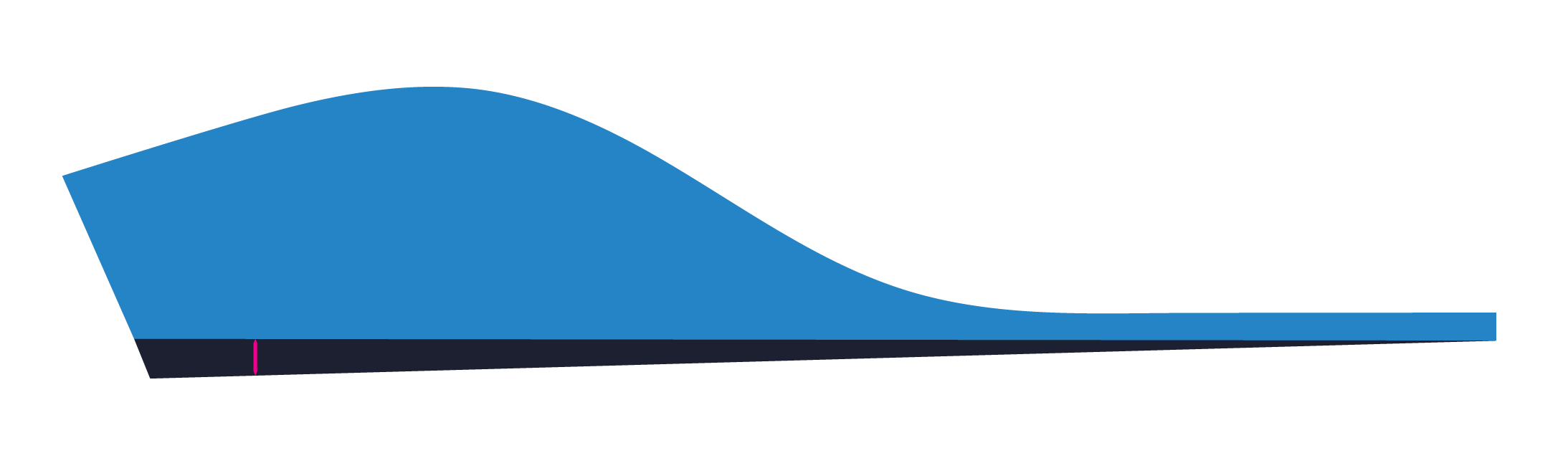
The Extrinsic Heel Lift will be tapered from the proximal heel to no thickness in-line with the metatarsophalangeal joints. The specified thickness will be measured from the heel centre as indicated by the pink line in the image below.
Tapered to Sulcus
The Extrinsic Heel Lift will be tapered from the proximal heel to no thickness in-line with the sulcus. The specified thickness will be measured from the heel centre as indicated by the pink line in the image below.
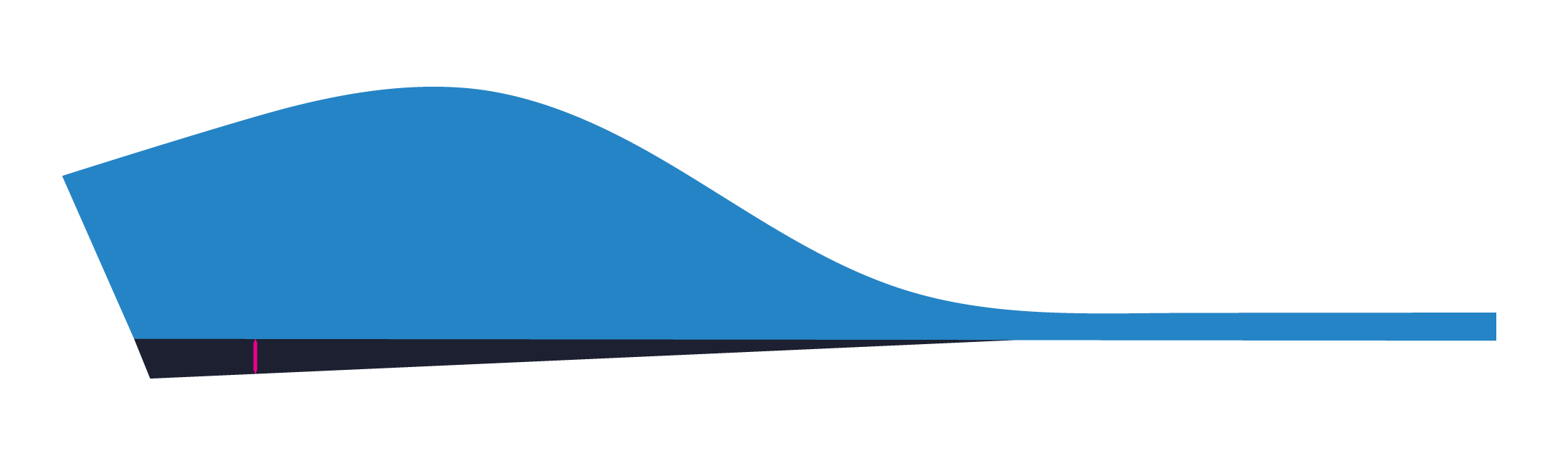
Tapered to Distal Edge
The Extrinsic Heel Lift will be tapered from the proximal heel to no thickness at the distal edge of the orthosis. The specified thickness will be measured from the heel centre as indicated by the pink line in the image below.
The Gait Plate option allows a user to request a polypropylene plate of a specific thickness be adhered to the plantar surface of the orthosis.
Gait Plates are commonly used in paediatric cases where there is a rotational deformity that is effecting the lower limb.
| Available Selection | Available Materials |
|---|---|
| In-Toe | Polypropylene 2.0mm Polypropylene 3.0mm Polypropylene 4.0mm |
| Out-Toe |
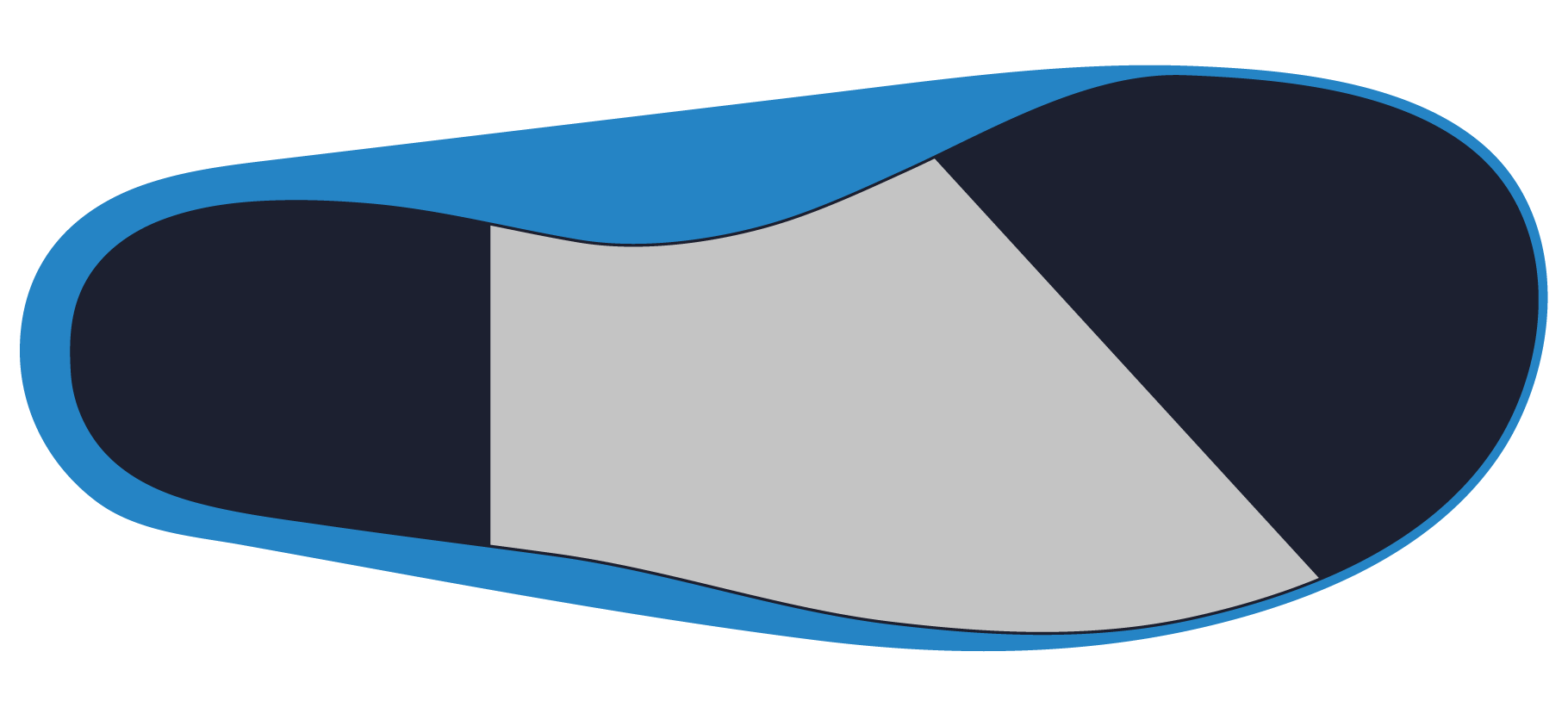
In-Toe
The Gait Plate will be manufactured for an in-toeing gait pattern. The Gait Plate will start proximal to the 1st metatarsophalangeal joint and then extend distal to the 5th metatarsophalangeal joint.
Ganjehie (2017) found that In-Toe Gait Plates can be used to improve gait appearance in children with in-toeing gait pattern due to excessive femoral anteversion.
Out-Toe
The Gait Plate will be manufactured for an out-toeing gait pattern. The Gait Plate will start proximal to the 5th metatarsophalangeal joint and then extend distal to the 1th metatarsophalangeal joint.